For decades, the omega-3 conversation went like this: the research is positive, take a supplement, you're sorted. The ORIP Trial — the world's largest randomised trial of omega-3 in pregnancy — changed the conversation. Here's what it actually showed, and why it's the reason testing exists.
The trial design
ORIP stands for Omega-3 to Reduce the Incidence of Preterm Birth. Led by Professor Maria Makrides and the team at SAHMRI, published in the New England Journal of Medicine in October 2019, it enrolled 5,517 pregnant women across multiple Australian centres.
Half were randomised to receive 900 mg/day of DHA-rich fish oil from the second trimester. Half received a vegetable-oil placebo. Standard randomised, double-blind, placebo-controlled design — the gold standard for clinical research.
The primary outcome was early preterm birth: babies born before 34 weeks of gestation. The kind of preterm birth that matters most clinically, with the highest rates of serious complications and the longest lasting impact on both baby and family.
The headline finding
Across the whole trial population, the difference between groups didn't reach the statistical threshold the team had pre-specified. On its face, that looked like a null result.
But the more interesting finding was buried in the subgroup analysis — and it was the part that changed everything.
When the team divided women by their baseline DHA status (measured at trial entry), they found that women with low DHA early in pregnancy (≤ 4.1% of red blood cell fatty acids) showed a substantial reduction in early preterm birth when they received the higher-dose supplement.
Women with already-adequate DHA at baseline did not show the same benefit. The supplement gave them no detectable advantage on the primary outcome.
The Simmonds 2020 follow-up
A year later, Simmonds and colleagues published an exploratory analysis in BJOG looking specifically at the relationship between baseline omega-3 status and early preterm birth across the trial population. The pattern was clear: benefit concentrated in the low-baseline group, and a hint that supplementation in women with already-adequate levels may not have been entirely neutral.
Why this is different from how we usually think about supplements
Most over-the-counter supplements are marketed on the assumption that more is better, or at worst neutral. "Take it daily, your levels will be supported, no harm done".
Omega-3 in pregnancy doesn't fit that model. The science says: if you need it, the benefit is large and clinically meaningful. If you don't, the case for taking it isn't there. And the published evidence at higher levels in adequate-baseline women is less reassuring than the marketing implies.
This isn't a problem specific to fish oil, krill, or algae — it's the same logic regardless of source. It's a precision-medicine problem. Different starting points need different interventions. The way you find out your starting point is by measuring it.
What this changed in clinical practice
The ORIP and Simmonds findings drove the SAHMRI Omega-3 Test-and-Treat Program — statewide implementation in South Australia from 2021, becoming routine antenatal care from 2026. From this year, every pregnant woman in SA gets her omega-3 status measured as part of her routine blood work, and supplementation is targeted to those who need it.
This is one of those rare cases where research evidence has translated into routine clinical practice on a defined timeline. National scale-up is underway.
What it means outside pregnancy
The ORIP findings were specific to pregnancy and preterm birth. But the underlying logic — that the right intervention depends on the starting level — generalises.
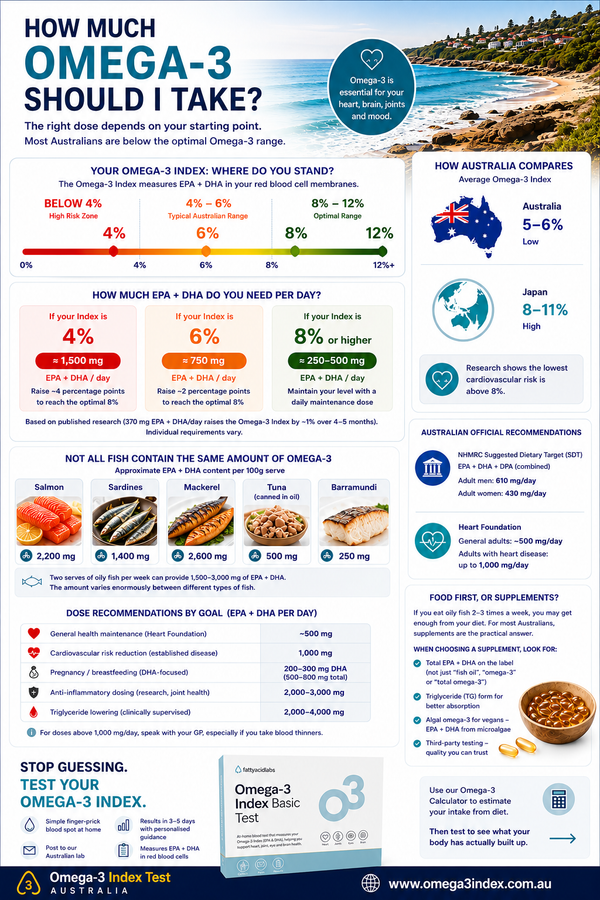
If you're at 4% Omega-3 Index and considering an omega-3 supplement (fish oil, krill, or algae-based), the published evidence supports that. If you're already at 9%, the case for adding more is much less clear. "More is better" isn't how the evidence actually reads. Targeted is better.
That's the case for testing first — in pregnancy, where the evidence is strongest, but also more broadly. Cheap (a single test), quick (a finger-prick at home), and the only way to know what you're actually optimising.
Test before you supplement
One finger-prick. Posted to your door. Results in 3–5 days. So you know what you actually need.
See our tests →References
- Makrides M, Best K, Yelland L, McPhee A, Zhou S, Quinlivan J, et al. A Randomized Trial of Prenatal n-3 Fatty Acid Supplementation and Preterm Delivery (ORIP Trial). New England Journal of Medicine. 2019;381:1035-1045.
- Simmonds LA, Sullivan TR, Skubisz M, Middleton PF, Best KP, Yelland LN, et al. Omega-3 fatty acid supplementation in pregnancy — baseline omega-3 status and early preterm birth: exploratory analysis of a randomised controlled trial. BJOG. 2020;127(8):975-981.
- Middleton P, Gomersall JC, Gould JF, et al. Omega-3 fatty acid addition during pregnancy. Cochrane Database of Systematic Reviews. 2018;11:CD003402.
- Best KP, Northcott C, Simmonds LA, et al. Feasibility, Implementation and Early Adoption of an Omega-3 Test-and-Treat Program. Medical Journal of Australia. 2025.
Know your number.
A simple at-home finger-prick test, posted to your door. Find out where you actually stand on omega-3.
See our tests